Medical Oncologist- Lung cancer, thymic & NUT carcinomas. Head of Clinical Research @GustaveRoussy, Head of Scientific Chairs Council @EORTC. Tweets are my own.
Ultra-Low-Dose nivolumab (20 mg, 6% of the FDA-approved flat dose) does the job in Head and Neck Cancer. 1-year OS improved, from 16.3% to 43.4%, HR 0.545; P = .0036. Fantastic trial! De-escalation IO studies are highly needed.
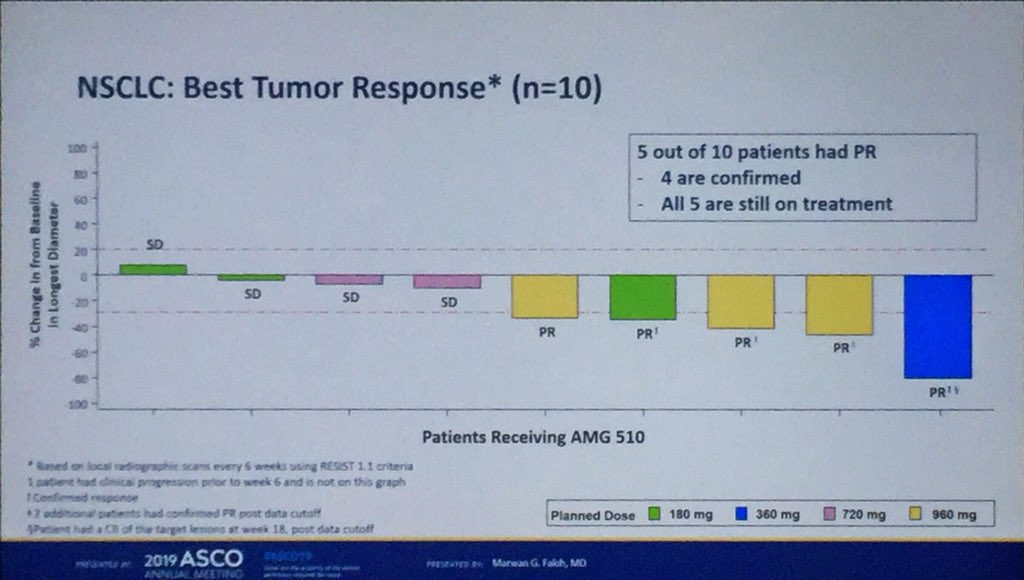
Gooooaaaaaal! KRAS G12C (13% of lung cancer) can be targeted! 5 responses out of 10 pts with heavily pretreated KRASmut NSCLC (1 to be confirmed), only 1 PD. Some long responses. Good safety profile. Probably the most impressive results for lung cancer at #ASC019.
The KRAS inhibitors familly grows : G12D mutation is targeted by MRTX1133 with convincing preclinical data on orthotopic models, in particular of pancreatic cancer. #targets21
Accumulative publications showing that immunotherapy is more potent when given early in the day. Time to change our practice and give our IOs in the morning? At least until evidence of a circadian biology supporting the hypothesis & availability of data from phase III trials?
Stop pembro after 2 years?
In 43,359 pts that received up-front pembrolizumab for an advanced NSCLC, continuation beyond 2 years was not associated with better OS than a fixed 2-year treatment, HR = 0.97 [0.75–1.26] p = 0.95.
@arousseaumdsciencedirect.com/science/articl…
Resistance post osimertinib: acquired fusion in 16% of the NSCLC, all can be targeted (RET, FGFR3, BRAF, ALK)!!
Much more fusions than reported because most studies at resistance are on ctDNA.
16% is what we find with RNAseq on a fresh tissue biopsy (n=31). 1526P #ESMO2019
MET IHC is a strong predictive factor for the efficacy of amivantamab + lazertinib in pts with EGFRmut NSCLC, independently of the resistance mechanism to osimertinib. PFS 12.2/4.2mo in MET+/-. Might be useful if the 1st line setting becomes crowded (FLAURA2, MARIPOSA…). #ASCO23
Welcome to 4th Gen EGFR inhibitors!
BLU-945 hits triple mutant EGFR+/T790M/C797S, alone and in combo (fig B and A, adapted from 1296P).
Triple mut are seen in EGFRmut NSCLC treated with 1st/2nd Gen followed by osimertinib (usually T790M is lost after osi 1st line). #ESMO20#LCSM
LIFETIME osimertinib after a treatment with curative intent?
In pts with EGFRmut stage III NSCLC, chemo-radiotherapy can CURE pts.
Were pts in LAURA properly staged by petscan/brain RMI?
Why not using MRD to select patient?
Strong concerns when OS is not positive. #ASCO24
Lung cancer is not the only solid tumor sensitive to KRAS G12C inhibitors. Adagrasib is potent in 10 patients with pretreated pancreatic cancer: 5 responses (including 1 unconfirmed response). #Targets21
Adjuvant pembrolizumab improves Disease Free Survival in pts after complete resection of stage IB-IIIA Non-Small Cell Lung Cancer HR=0.76 (IC95 0.63-0.91), including subgroups PD-L1 neg (HR=0.78) or stage IB (HR=0.76). PEARLS study by @EORTC @ETOP_eu. @myESMO virtual plenary.
PULSE, a @GustaveRoussy pragmatic trial that de-escalade the dose of immunotherapy in patients with lung cancer is activated in France!
Goals: increase patient’s quality of life and decrease financial toxicity.
Will also open in Spain. DM if interested to join!
Immuno in first line NSCLC
Perfect summary from @peters_solange#ESMOacademy2018
Chose the best regimen patient by patient, based on activity, toxicity, patient’s preference.
ADCs for SCLC: highly needed!
DS-7300, an ADC against B7-H3, induced a confirmed response in 10/19 (53%) patients. DoR : 5.5 months. Update of the subgroup analysis from the Phase I/II study that enrolled 147 patients. #ESMO22